
Anterior Cruciate Ligament (ACL) injuries are one of the most common sporting injuries, especially in sports that involve sudden changes of direction such as soccer, netball, and rugby.
What is the ACL?
The ACL is one of four stabilising ligaments in the knee. It runs from the shin bone (tibia) to the thigh bone (femur), acting like a rope that prevents the shin from sliding forward and provides stability for twisting and pivoting movements.

How Do ACL Injuries Happen?
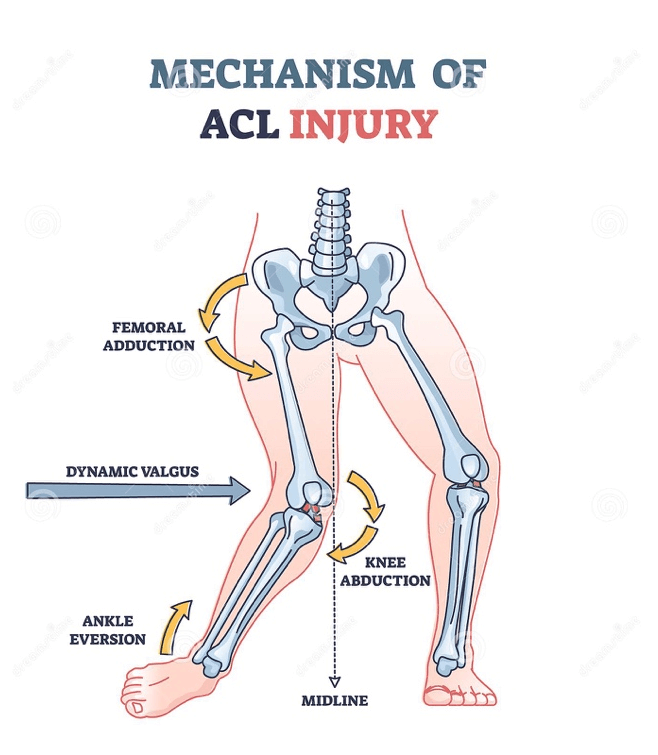
The ACL is at high risk of rupture or tear during:
Pivoting quickly on a planted foot
Sudden stops or changes of direction
High impact to the knee with the foot fixed
Most people describe hearing a “pop” followed by pain and swelling within hours. Sometimes the ACL tears in isolation, but often other knee structures (like the meniscus) are also injured, complicating rehab and treatment.
Treatment Options
There’s no single answer to the “best” treatment — it depends on your lifestyle, sport, and personal goals.
Surgical ACL Reconstruction
Surgery is still the most common treatment. It involves creating a new ACL from a tendon (your hamstring, patella, or quadriceps) or a donor graft. It’s usually a day surgery via arthroscopy.
Rehab starts immediately after surgery, with goals to reduce swelling, regain quadriceps activation, and restore full knee extension.
Running: typically around 12 weeks (straight line only)
Return to sport: usually 12 months, after a full sport-specific rehab program
Conservative (Non-Surgical) Management
Some people can successfully manage an ACL injury without surgery. Instead of repairing the ligament, physiotherapy strengthens the surrounding muscles to stabilise the knee. This approach is becoming more widely recommended for people with:
Isolated ACL tears (no other major damage)
Lower physical demands or no desire to return to high-pivot sports
With the right rehab, conservative treatment can allow people to return to activity and avoid the risks associated with surgery. However, it requires strict adherence to physiotherapy to prevent further injury.
Initial Management
Whether you choose surgery or not, rehab begins immediately after diagnosis (MRI or physio assessment). The first steps include:
Reducing pain and swelling
Activating quadriceps muscles
Improving balance and range of motion
Gentle exercise, ice, and anti-inflammatories
So… Which Approach Is Best?
The short answer: it depends.
Athletes returning to high-risk sports often need surgical repair.
People with lower activity levels may succeed with conservative rehab.
Additional injuries to the knee (like meniscus tears) often make surgery the better option.
The best plan is an individual one — made in consultation with your physiotherapist and specialist.
📞 Have questions about ACL injuries or treatment options? Call Mudgee Physio on 6372 4033 to book an appointment with one of our physiotherapists.


